
by Prof Dr M Sultan Khuroo
Most epidemiologists caution against raising alarm over Human Metapneumovirus (HMPV), viewing it as manageable. However, they stress the importance of proactive measures, urging countries to capitalise on opportunities to enhance preparedness for potential health crises. Vigilance and readiness remain key to mitigating risks and ensuring swift responses to any unforeseen challenges.
Five years after COVID-19 emerged from Wuhan, and evolved into one of the worst pandemics, another threat is looming from China. Hospitals in China are crowded with patients wearing masks and coughing, and videos on social media depict scary scenes. Human Metapneumovirus (HMPV) is believed to cause these respiratory infections. The World is watching this evolving situation with concern. However, China CDC surveillance data on acute respiratory infections up to December 29, 2024, acknowledged a surge caused by seasonal influenza, rhinovirus, respiratory syncytial virus (RSV), HMPV, and mycoplasma pneumonia, particularly in northern China. All this has been attributed to a routine winter seasonal spike. The authorities refuted the occurrence of an unusual outbreak, overwhelmed healthcare and emergency declaration or responses, and reported that hospital utilisation is lower than last year. WHO continues to monitor respiratory illnesses at global and country levels and has not found any unusual outbreak pattern in China.
Acute Respiratory Infections (ARIs)
Acute respiratory infections (ARIs) are a significant health problem worldwide, especially in developing countries. These are classified as Acute Upper Respiratory Infections (AURIs) and acute lower respiratory infections (ALRIs). In 2021 alone, there were an estimated 12.8 billion new episodes of ARIs.
ARIs are responsible for almost 20 per cent per cent of all deaths of children aged less than 5 years worldwide. Globally, 20 per cent of children under five who die from ARIs live in developing countries. Risk factors include poverty, poor nutrition, overcrowding, and lack of healthcare facilities. The etiological spectrum of ARIs is broad and includes pathogens of viral and bacterial origins.
Among patients with positive viral cultures, the common viruses include Influenza virus (28.5per cent), respiratory syncytial virus (RSV, 16.8per cent), human rhinovirus (16.7per cent), and human metapneumovirus (HMPV, 4.1per cent). Among positive bacterial cultures, the common bacteria, among others, include Streptococcus pneumonia (29.9 per cent) and Mycoplasma pneumonia (18.6 per cent).
In many northern hemisphere countries, trends in ARIs increase in winter months. Seasonal epidemics of respiratory pathogens such as seasonal influenza, RSV, HMPV, and mycoplasma pneumonia typically cause these increases. Surveillance data shows increased rates of influenza-like illness (ILI) and ARIs above baseline levels in many regions, following usual seasonal trends. Influenza activity is notably high across Europe, Asia, and the Americas. RSV trends vary, with increases in North America but decreases elsewhere. The World Health Organisation (WHO) advises maintaining surveillance and taking precautions, such as staying home when sick, wearing masks in crowded spaces, and practising good hygiene. WHO continues to monitor global respiratory illness trends and provides updates as needed.
Human Metapneumovirus (HMPV)
Discovery: In 2001, Dr van den Hoogen and her colleagues discovered HMPV in the Netherlands from the respiratory secretions of 28 young children with respiratory illnesses using the RAP-PCR (RNA arbitrarily primed PCR) technique. The human metapneumovirus (HMPV) was named because of its genetic similarity to the avian Metapneumovirus. Serologic studies of antibodies against HMPV indicate that the virus is not new and has circulated in humans for at least 50 years before 2001.
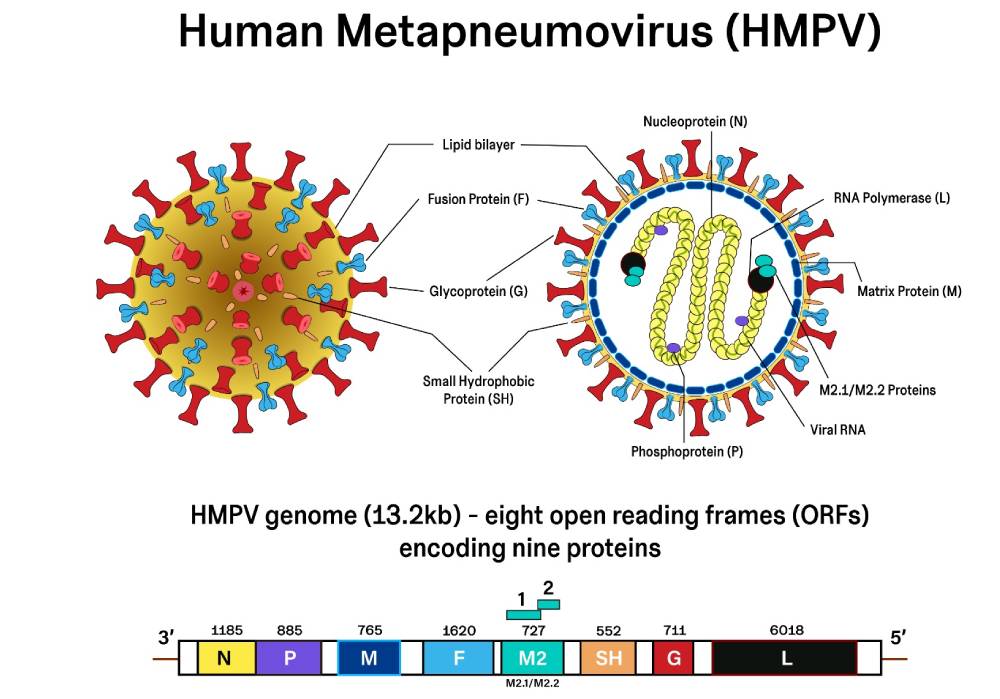
Virology (Fig): The HMPV is a single-stranded, negative-sense RNA virus with a genome of about 13.2 kilobases (kb) in length. The genome contains eight genes (open reading frames, ORFs), with an order of genes as 3′-N-P-M-F-M2-SH-G-L-5′. It encodes nine structural proteins: N (Nucleoprotein, helps in the formation of nucleocapsid), P (Phosphoprotein, helps in viral replication and transcription), M (Matrix protein, helps in viral assembly and budding), F (Fusion protein, helps in the fusion of the virus in to host cell), M2-1 and M2-2 protein (helps in transcriptional regulation), SH (Small hydrophobic surface protein with unclear function), G (Major attachment glycoprotein), and L (Major polymerase subunit).
HMPV belongs to the family Paramyxoviruses, subfamily Pneumovirinae, and genus Metapneumovirus.
The HMPV virion is pleomorphic, varying in size from 150 nm to 600 nm. The particle has an outer lipid bilayer with three embedded proteins: the F protein (a trimer), the G protein (a tetramer), and the small SH protein (a pentamer), forming spikes of approximately 13-17 nm. The viral matrix (M) lies underneath the lipid bilayer and encapsulates a Ribonucleoprotein complex (Nucleocapsid). The viral RNA is wrapped by a nucleoprotein (N) and associated with phosphoprotein (P), large RNA-dependent RNA polymerase (L), and two other matrix proteins (M2-1 protein and M2-2 protein).
HMPV is divided into two genotypes, A and B, and each genotype is further divided into subgroups: A1, A2a, A2b, B1, and B2. Apart from the five agreed-upon subtypes, novel subtypes of HMPV, namely A2c, A2b1, and A2b2, have been proposed.
Replication: The HMPV infects the epithelial cells lining the nose, throat, larynx, bronchi, and lungs. The virion attaches to the cell surface by the G protein and, with the help of the F protein, fuses with heparin sulphate receptors. The virus then enters the cell. The N, P, and L proteins separate from viral RNA and bind to form the polymerase complex, which transcribes the viral RNA into messenger RNA (mRNA). The host’s ribosomal machinery translates the mRNA to produce viral proteins for replication and assembly.
At the same time, viral replication occurs to make a viral genome encapsulated by nucleoprotein (N protein) to form nucleocapsid complexes. The P protein acts as a co-factor to stabilise the L protein, allowing the formation of a nucleoprotein complex during virus replication. M2-1 and M2-2 protein plays a significant role in regulating virus replication and decreasing host innate immunity. The M proteins play a crucial role in virus assembly and budding by interacting with the RNP complex. The virion buds out of the cells with F, SH, and G proteins exposed on the outer side of the membrane.
Host immune response: HMPV antagonises the cellular responses of Toll-like receptors, retinoic acid-inducible gene-like receptors, and other signalling molecules. Infection also interferes with dendritic cell activity and reduces the antigen-specific T-cell response. This leads to incomplete virus clearance and the chance of re-infection.
Pathogenesis: Mucus production is a common feature during HMPV infection. Mucin is a significant component of mucus and could impact the host’s response to infection. HMPV induces a reaction of chemokines and cytokines such as IL-6, IFN-alpha, TNF-alpha, IL-2, and macrophage inflammatory proteins, leading to perivascular inflammation and inflammation in the epithelial cells of the airways. In addition, viral cytopathic effects lead to damage to the epithelial layer.
Epidemiology: HMPV primarily infects humans, and there is no animal reservoir. The virus infects the upper and lower respiratory tract, including the nose, throat, and lungs. Infection occurs primarily in young children, and nearly all children below 5 years old are exposed to it. HMPV is the cause of AURIs in 15per cent of children and ALRIs in 12per cent of children with a mean age of 11.6 months. Of the ALRIs, the virus was associated with bronchiolitis in 59 per cent of cases, pneumonia in 8 per cent, croup in 18 per cent, and an exacerbation of asthma in 14 per cent. Thus, HMPV is a leading cause of respiratory tract infection in the first years of life, with a spectrum of diseases similar to RSV.
In addition, due to incompletely protective immune responses or infection with a new genotype, reinfection occurs in high-risk groups, including older adults over 65, people with low immunity, chronic respiratory disorders, and premature infants. The etiological spectrum of ARIs in adults includes Influenza A (6.5 per cent), RSV (6.1 per cent 0 and HMPV (4.5 per cent). Average annual hospitalisation rates for HMPV were 1.8/10,000 residents in adults aged 50–65 years and 22.1/10,000 in adults >65 years. Compared to patients with influenza, patients with HMPV infections were older, had more cardiovascular disease, and were more likely to be vaccinated with flu. HMPV infection is a seasonal disease that occurs typically in the winter and early spring, similar to RSV infection.

Transmission: HMPV is most likely spread from an infected person to others through aerosol from secretions from coughing and sneezing. It can also spread by close personal contact, such as touching or shaking hands or sharing closed, poorly ventilated spaces. The virus can survive on surfaces for several hours, which may cause indirect transmission. Thus, touching objects or surfaces with viruses and then touching the mouth, nose, or eyes can transmit the infection. Since the virus is thought to spread through coughing, sneezing, or touching objects, surfaces, or hands that have viruses on them, the risk of catching or transmitting it can be reduced by taking similar precautions to those that prevent the spread of other respiratory pathogens, such as influenza.
Clinical profile: The incubation period of HMPV infection is 3 to 6 days, and the uncomplicated illness lasts a week or two. The respiratory tract is the primary target. The clinical spectrum is determined by the individual’s age, health condition, and immune status and includes upper respiratory infection, lower respiratory disease, severe clinical syndromes, and secondary infections. The illness is generally indistinguishable from respiratory infections caused by other respiratory viruses like Influenza, RSV, and even COVID-19. This similarity can make initial diagnosis challenging without specific testing.
In most cases, the virus infects the nasal mucosa, throat, and larynx (Upper respiratory tract) and presents as a cough, fever, nasal congestion, sore throat, and dry cough. These symptoms are mild and resolve on their own within a week or two. However, in severe cases, particularly among vulnerable populations, HMPV can involve bronchi, bronchioles, and lung parenchyma (lower respiratory tract) and may cause bronchitis, bronchiolitis, and pneumonia. Patients with bronchitis present with productive cough, phlegm, and chest discomfort. Bronchiolitis is common in infants and young children and causes inflammation, swelling, and narrowing of small airways. It presents as cough, wheezing, difficulty in breathing, and hypoxia. Sick patients may need hospital admission and ventilator support. HMPV pneumonia can present with fever, severe cough, chest pain, shortness of breath, fatigue, and hypoxia. HMPV infections cause the exacerbation of asthma and flare-up of pre-existing COPD. Otitis media is known to occur with HMPV.

Diagnosis: Patients with HMPV infection need clinical evaluation of the severity of the disease based on symptoms and clinical assessment. If bacterial infection is suspected, routine blood counts are done. Patients suspected of lung involvement need a chest X-ray and CT scan to evaluate possible pneumonic illness. Bronchoscopy and bronchial lavage may be indicated in cases with severe lung disease. Most patients have mild disease, indistinguishable from other viral infections, namely Influenza, RSV, and COVID-19, and do not warrant specific diagnostic tests for HMPV.
However, such tests are needed in severe cases where antiviral treatment is required and if surveillance of HMPV is justified. It’s worth noting that testing for HMPV is generally reserved for patients experiencing significant respiratory distress, such as those at risk for complications, including young children, older adults, or individuals with weakened immune systems.
Early and accurate diagnosis is crucial for guiding treatment and preventing further complications. The virus’s culture is complex as it grows slowly in conventional media and has little cytopathic effects. The most sensitive method is to detect viral RNA from nasal and throat swabs and sputum by NAAT, such as RT-PCR, with results available in a few hours. HMPV antigen detection with anti-HMPV antibodies by indirect immunofluorescence or ELISA is less sensitive and not routinely done. HMPV antibodies in blood by ELISA are useful for seroprevalence studies and determining previous exposure to infection.
Mortality: Patients with HMPV and RSV lower respiratory tract disease had similar rates of hypoxemia and mechanical ventilation at any time during the episode. In patients with severe pneumonia and respiratory failure, mortality rates by day 100 after diagnosis were identical between patients with HMPV and RSV (43 per cent versus 43 per cent), and deaths related to the actual viral infection were also similar (39 per cent versus 35 per cent).
Treatment: To date, treatment of HMPV infection is supportive. This includes over-the-counter medications such as analgesics and decongestants. Hydration and a room humidifier may help. Oxygen therapy is indicated if breathing is difficult. A short course of steroids may reduce bronchial inflammation and edema and is worth trying in select cases. Of course, sick patients with respiratory failure need to be recognized and hospitalized for ventilatory support. Antibiotics are not generally recommended unless a primary or secondary bacterial infection is suspected or proven on sputum culture.
Ribavirin plus intravenous immunoglobulin has been found to have in vitro antiviral properties and has shown clinical improvement in sick patients with HMPV infection. However, there are no clinical trials with this form of treatment. Ribavirin, both oral and nebulised therapy, has been recommended. Targeting fusion proteins with inhibitory peptides is being investigated, and it shows promise in vitro and animal studies. However, none of these are in the clinical domain. Other innovative methods under study include monoclonal antibodies and several vaccines, which have shown promise in vitro and animal studies.
No vaccines are currently available for HMPV infection. Several candidate vaccines have been tested and are under development. These include mRNA-based vaccines (mRNA-1653, mRNA-1345, and mRNA-1365 from Moderna) and ALVIR106 multi-virus T-cell therapy by AlloVir.
Prevention: Preventing HMPV infection is similar to preventing other respiratory illnesses. These include wearing a mask in crowded or poorly ventilated spaces, improving ventilation where possible (such as by opening a window for airflow), cleaning hands regularly and thoroughly with either soap and water or an alcohol-based hand rub, and avoiding touching eyes, nose, or mouth without washing hands first. A strong immune system can also help ward off infections. Eating a balanced diet, exercising regularly, and sleeping properly can help.
When someone is sick, they can avoid making others sick by staying at home, covering their nose and mouth with a tissue or bent elbow when coughing or sneezing, wearing a mask when around other people, improving ventilation, especially in shared spaces, regularly cleaning hands and disinfecting frequently touched surfaces.
No vaccine is currently licensed against HMPV, but research is ongoing.
Looming Threat or False Alarm:
Five years after the COVID-19 pandemic, the world faces another threat from another virus, namely HMPV. Several factors have made the global community quite concerned about the situation. Hospitals in China are crowded with patients wearing masks and coughing, and videos on social media depict scary scenes. These scenes resemble those seen in China before the COVID-19 pandemic erupted in Wuhan, China.
Human Metapneumovirus (HMPV) is believed to cause these respiratory infections. Both SARS-CoV-2 and HMPV share many common features, which include:
- Both are RNA viruses.
- Both viruses can mutate, and new strains emerge.
- The mode of transmission is similar.
- Both show seasonal trends with higher occurrence in winter and early spring.
- Both cause Acute respiratory infections (ARIs) and tend to cause severe illness in the elderly and immunocompromised.
- As happened with SARS-CoV-2 in 2019, cases of HMPV have been detected in several neighbouring countries, including Malaysia, Hong Kong, and Kazakhstan.
However, critical evaluation shows significant differences between SARS-CoV-2 and HMPV. SARS-CoV-2 was a new virus introduced in humans with no previous exposure and immunity. HMPV was discovered in 2001 but has been shown to exist at least 50 years before that. Children under five years old have HMPV antibodies and thus have partial immunity against re-infection. Therefore, the risk of a pandemic from HMPV is low.
HMPV mutates and changes over time, with new strains emerging; the changes are gradual and based on previously circulating strains. Pandemics occur when a new virus enters the human population, like SARS-CoV-2, or in the case of influenza, when a new strain of the virus emerges that can spread quickly from person to person and for which humans have little or no immunity. There is no such possibility with HMPV.
Though social media has extensively covered the situation in China, the official reports from the China CDC and Government were utterly different. China acknowledged a surge caused by seasonal influenza, rhinovirus, RSV, HMPV, and mycoplasma pneumonia, particularly in north China. The authorities refuted the occurrence of an unusual outbreak, overwhelmed healthcare and emergency declaration or responses, and reported that hospital utilization is lower than last year. WHO continues to monitor respiratory illnesses at global and country levels and has not found any unusual outbreak pattern in China.
As mentioned above, the diagnosis of HMPV in several countries should not be a concern. ARIs show a seasonal trend in the north during winter and early spring. Several viruses cause such infections, and HMPV significantly contributes to them. So, surveillance will detect HMPV in cases of ARIs in most countries.
What is the way forward? Most epidemiologists believe not to ring the alarm bell. However, countries need to move forward and take advantage of opportunities to be prepared for any eventuality. As in the COVID-19 pandemic, the most important thing is to have surveillance and testing facilities. Any outbreak, even if seasonal, must be reported and preventive measures implemented. Also, public education and advice need to be strengthened so that unnecessary panic can be controlled.
(Leading gastroenterologist, Dr Khuroo is a scientist, who headed SKIMS earlier.)













