
by Prof Mohammad Sultan Khuroo
The patients carrying the peculiar disease were from tribal populations living in the low mountainous regions of Kashmir or adjacent border areas and had livelihoods closely tied to the forests, which they frequently visited over the years.
Kashmir is emerging as an endemic zone for Alveolar echinococcosis (AE) and poses a public health threat (Fig 1). AE is caused by the larval stages (metacestode) of cestode, the fox tapeworm Echinococcus multilocularis (E. multilocularis). The disease primarily affects the liver and causes bulky tumours, which infiltrate centrally to the vascular and biliary system and peripherally to the liver capsule and adjacent organs. The tumours metastasize to the lungs, brain, and bones. Left untreated, the disease is uniformly fatal within eight years.
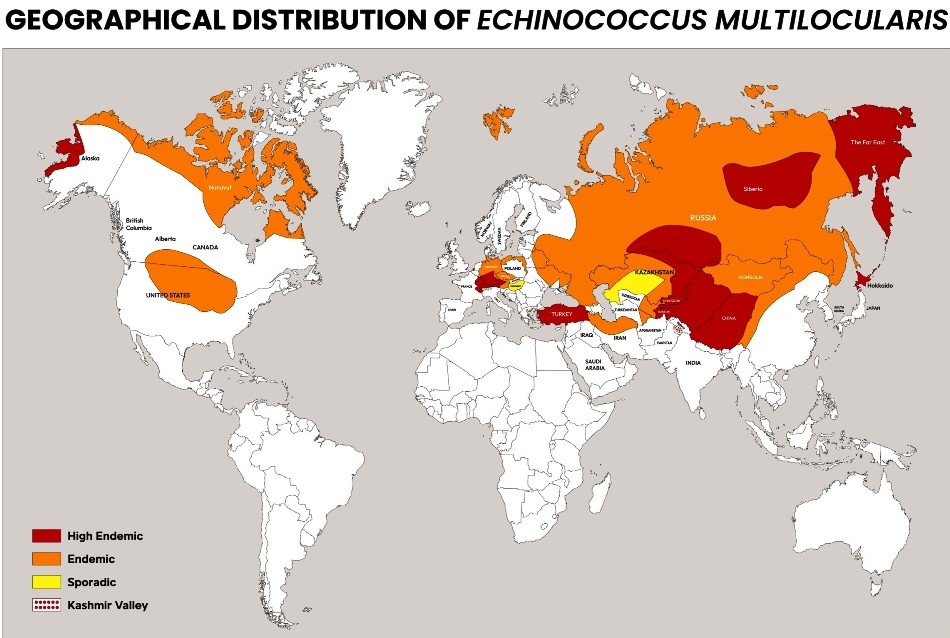
E. multilocularis, the causative agent of AE, is distributed across the northern hemisphere, including Northern Japan, north of Russia, northwest China, central Asia, central and northern Europe, the north-central United States, north-western Alaska, and northwest Canada (Fig 2). AE is a growing global public health threat, with approximately 18,235 new cases recorded annually worldwide, resulting in a disease burden of 666,433 disability-adjusted years (DALYs). China accounts for 91 per cent of these cases, with the disease highly endemic in seven counties of northwest China, where the disease prevalence exceeds 3 per cent in the general population. A significant increase in human infections has occurred in Europe in recent years. The eggs of E. multilocularis require specific environmental conditions, such as high humidity and dense vegetation, to survive and spread, limiting the infection to the Northern Hemisphere.
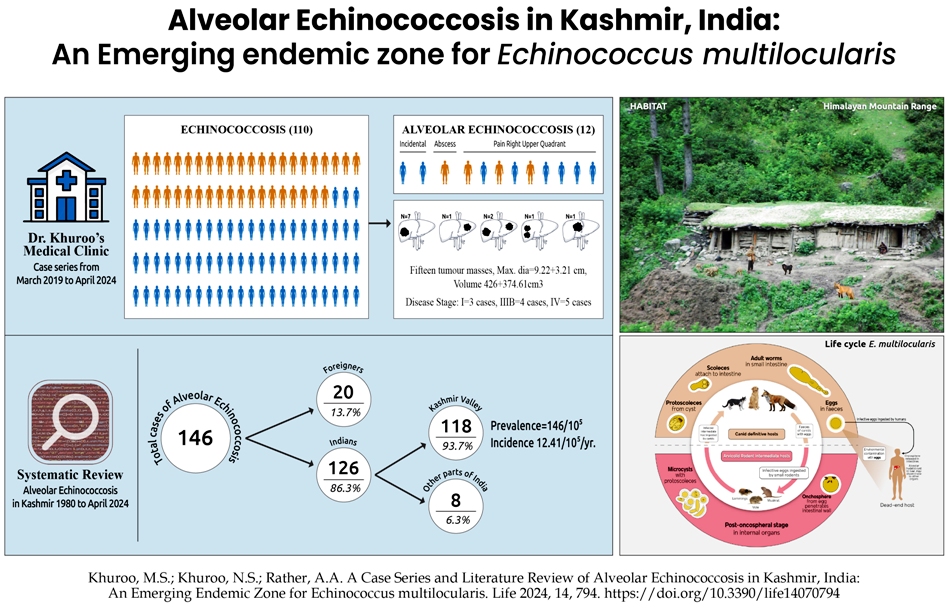
Adult worms of E. multilocularis live in the intestinal tract of canids, including red foxes, arctic foxes, and coyotes (Fig 1). The adult worm is 3 to 5 mm in size and has a scolex, a short neck, and three proglottids (segments). The gravid proglottid contains an average of 823 eggs passed with faeces (Scat). Arvicolinae, a subfamily of rodents, including the voles, lemmings, and muskrats, serve as intermediate hosts. They ingest eggs from contaminated food, water, and soil. The eggs hatch in the gut lumen and release a six-hooked oncosphere that penetrates the intestinal wall and migrates through the circulatory system into the liver. The oncosphere develops into a multi-chambered (multilocular), thin-walled (alveolar) hydatid cyst that proliferates by successive outward budding of germinal layers to form numerous vesicles, embedded in the immune reaction of the host (granuloma, fibrosis, and necrosis). Protoscoleces develop within these vesicles. The definitive host becomes infected by ingesting the metacestode-containing organ of the infected intermediate host. After ingestion, the protoscoleces evaginate, attach to the intestinal mucosa, and develop into adult worms in 32 to 80 days. Man is an accidental dead-end intermediate host and acquires infection by ingesting eggs from food, water, or soil or by direct contact with the definitive host. The cyst vesicles in man are sterile and lack protoscoleces.

Human AE presents as an expanding, infiltrative liver tumour with local and distant metastases (Fig 3). The liver tumour may be detected incidentally on routine liver imaging and often presents as pain in the right upper quadrant. The tumour may show central necrosis and resemble a liver abscess. Involvement of centrally placed bile ducts causes biliary obstruction, episodes of cholangitis, liver abscesses, sepsis, and multiorgan failure. Invasion of the portal venous system and hepatic outflow tract leads to portal hypertension and Budd Chiari syndrome. Infiltration to adjacent organs, namely the heart, adrenals, diaphragm, mesentery, and pleura, causes specific organ dysfunction. Diffuse liver disease can cause liver failure. The tumour metastases to the lung present as lung nodules or infiltrative lung disease, to the brain as mass lesions, and to bones with tumours and fractures. Left untreated, the disease is fatal within a few years.
Diagnosis
Diagnosis and evaluation of AE is complex and multidisciplinary. Given the slow growth of the lesion and non-specific clinical presentation, a high degree of clinical suspicion is needed. Multimodal imaging is the cornerstone for clinching a diagnosis (Fig 4). Ultrasound and CT scans are good for detecting liver tumours with calcifications and tumour characteristics, extension, and invasion.
MRI is more specific as it helps to evaluate disease activity on T2WI, diffusion-weighted characteristics on T1WI, and biliary tract on MRCP. PET scans are very specific as FDG uptake is markedly increased at the lesion’s periphery determining the metabolic activity (viability) of AE scoleces. Serology based on Em2plus-based ELISA is sensitive & specific and often confirms imaging results. Histological findings include strongly PAS-positive microcysts, extensive necrosis, granulomatous inflammation, and calcification. DNA identification methods are now routinely used on biopsy or fine-needle cytology specimens to diagnose AE in patients with unusual imaging aspects and negative serology typified by immune-suppressed patients. In 2003, Kodama et al. proposed classifying AE lesions from type I to type V through MRI identification of the lesions’ solid and/or cystic portions. The presence of micro-cysts appears to be strongly correlated with PET-CT hypermetabolic activity around AE liver lesions and suggests disease with activity. The absence of micro-cysts with solid and large cystic tumours is often caused by old inactive lesions.
Because the growth pattern of AE resembles liver cancer, WHO, guided by TNM classification and staging, has proposed PNM classification to stage the disease and plan treatment. P represents parasitic mass in the liver and is divided into PX to P4, N describes the involvement of neighbouring organs, and M represents the occurrence of distant metastases. Based on the PNM classification, the disease is divided into four stages. Early localized diseases under stage I and II are amenable to curative liver resections. A 2-year chemotherapy is to be given, and serology with ultrasound is done every 6-24 months, and MRI or PET/CT every 2-4 years to watch for disease recurrence. The disease is considered healed after ten years without recurrence. Managing advanced local or distant disease under stages IIIA, IIIB, and IV is a complex clinical problem. Generally, radical surgery is done in select cases. Palliative surgery is discouraged. Long-term chemotherapy is the sole form of therapy and may arrest the progression of the disease. Patients with biliary and vascular complications often need interventional or surgical procedures. Liver transplantation and Ex-vivo liver resection liver transplantation are done with localized advanced disease.
Status in Kashmir
What is the status of AE in India? I reported the occurrence of AE for the first time in India in 1980. The patient was a 40-year-old male from Uri who presented with a large liver mass (18 x14 cm) with extensive necrosis and cavitations. The tumour had invaded IVC, blocking its ostium, causing Budd Chiari syndrome. The hepatic lesion had infiltrated into the right atrial wall, resembling an atrial tumour. The tumour involved the diaphragm and the left pleura as well. The patient died after surgery and had a diagnosis at autopsy. Only a few isolated cases were reported after this report, and AE was never a matter of concern in India. However, from 2012 onwards there have been several case reports and series from North India, including Kashmir.
Taking the lead from these reports, we planned several studies on AE in Kashmir, India. A prospective study was done to find the number of cases of AE from a cohort of 110 cases of echinococcosis seen at Dr Khuroo’s Medical Clinic (DKMC) from March 2019 to April 2024. Next, a systematic review was done to document cases of AE from Kashmir from 1980 to April 2024. We performed epidemiological studies to find the prevalence, incidence, and Disease Burden of AE in Kashmir. We debated whether the emergence of AE in Kashmir is a myth or reality and chalked out future directions to face the challenge.
The diagnosis of AE at DKMC was made based on clinical, serological, imaging, and histological findings. Echinococcus hydatid serology IgG was performed by ELISA using E. granulosus hydatid fluid. This is the first-line test for immunodiagnosis of both CE and AE, with a diagnostic accuracy of 95 per cent for AE. Imaging goals included i. Characterize the liver mass; ii. Define the extension of tumour masses toward the liver hilum involving the vascular system and biliary tract; iii. Extension toward the liver capsule, infiltrating the surrounding organs; iv. Parasite viability and activity at the onset and on follow-up; v. Tumour volume and future residual liver volume; vi. Distant metastases. For this, we employed ultrasound, CT, MRI, and PET scans with their selective advantages. With all that, confirmation of diagnosis needed histological proof of AE.
A prospective study of 110 echinococcosis cases at DKMC from March 2019 to April 2024 showed 98 cystic and 12 cases of Alveolar disease. Could the recent surge of AE in Kashmir be due to increased awareness, better healthcare facilities, and improved diagnosis? Based on our experience over the years, it seems unlikely. We have prospectively followed 229 echinococcosis cases from 1989 to 2005 at SKIMS, Srinagar, and 301 cases from 2005 to March 2019 at DKMC, Srinagar. All cases had CE, and no cases had AE. Thus, the emergence of AE is of recent origin and unlikely to be related to increased awareness of the disease or improved diagnosis.
Of the 12 cases of AE, there were 4 males and 8 females. The age of patients with AE at presentation was 46.58 ± 11.97 years (95 per cent CI 38.98 to 54.19). All patients were residents of Kashmir Valley. The patients belonged to tribal populations and lived either within the low mountainous regions of Kashmir (n = 4) or border areas of the valley adjacent to mountainous ranges (n = 8). The livelihood of these tribal populations was closely linked to forests, and they would often visit the forests over the years. Two patients were detected during routine ultrasound examinations for unrelated causes, while the remaining ten were symptomatic. The patients complained of pain in the right upper quadrant (n = 10), icterus (n = 2), generalized aches and pains with arthralgia (n = 1), and severe fatigue (n = 1). The mean duration of illness was 2.20 ± 1.79 years [95 per cent CI 1.09 to 3.30]. Physical examination in seven patients revealed firm to hard hepatomegaly with rounded margins and irregular surfaces. One patient presented with features of liver abscess due to massive tumour necrosis. Physical examination was unremarkable in the remaining four patients. Hydatid serology was strongly reactive in all cases.
(AE) in Kashmir
Liver imaging was remarkable as 15 liver tumours were seen. Nine patients had a single tumour while 3 patients had 2 tumours each in either lobe and different liver segments. Eleven tumours were placed in the right lobe, while four tumours were seen in the left lobe. The tumours were large and bulky, ranging from 5 cm to 15 cm, with an average of around 9 cm. Tumour volumes determined by contouring through HOROS software were an average of 426 cm3. Tumour characteristics were evaluated using various imaging methods, including greyscale ultrasound with Doppler, CT scans, and MRI. Six patients also had PET scans. Of interest, MRI T2WI classified tumour masses as Kodama I to III in 10 and Kodama IV & V in 5 lesions. PET scans in all six patients showed active disease by revealing a central hypometabolic (necrotic) component and rim of intense FDG avidity in the periphery resembling a Doughnut. The tumours had a strong invasive nature, as seen on imaging. Three peripheral masses had encased peripheral vascular and biliary elements. However, eight tumours had spread centrally to encase and invade vascular and biliary structures in the hilum. In addition, nine tumours had spread peripherally to involve the liver capsule, ligaments, diaphragm, and omentum. Right adrenal masses were detected in four patients. Lung metastases were seen in two patients and showed up as lung nodules and hilar lymphadenopathy. A PNM scoring placed the disease as stage III in 3 patients, Stage IIIB in 4 patients, and advanced stage IV disease in 5 patients. Histology of tumour material available on needle, laparoscopic, or resected material showed necrotic lesions with granulomatous inflammation and calcifications. However, the hallmark was the presence of slender, thin-walled vesicles with bizarre configurations stained strongly with PAS. These vesicles lacked the presence of protoscoleces, indicating these were sterile.
Three out of twelve patients had surgically curable early disease. Two patients had successful procedures, and a third patient refused surgery and was lost to follow-up. One patient with an infected necrotic abscess had tumour aspiration followed by surgical excision of the cyst contents. Eight patients with advanced disease were on chemotherapy with albendazole along with praziquantel. We have been impressed by the chemotherapy as patients had relief of symptoms, and tumour masses have regressed as evaluated clinically and on repeat ultrasound examinations. Of significance, none of these patients had disease progression. However, repeat MRI examinations at one year in one patient and MRI with PET scan at five years in another patient continued to show radiological evidence of active disease.
The Follow Up
Next, we did a literature search to find all cases of AE in India from 1980, when I described the first patient from India. For this, we used a systematic review under the PRISMA guidelines, which consists of a 27-item checklist and a four-phase flow diagram including Identification, Screening (selection criteria), Eligibility, and Inclusion. Diagnosis of AE was based on clinical, serological, imaging, and histological findings. Three search methods were employed, including published cases of AE, cases from Dr Khuroo’s Medical Clinic, and cases retrieved from other medical centres in Kashmir and North India.
Based on this, we found 146 patients of AE in India from 1980 to April 2024. Of these, 20 patients belonging to foreign countries visited tertiary care centres in North India for surgical procedures, including liver transplants. Of the 126 Indian nationals, 118 (93.65 per cent) were permanent residents of Kashmir. Of the 8 patients from other parts of India, 3 were Indian soldiers; one was a resident of Siliguri, west Bengal, and the other 4 were from different parts, namely UP, Rajasthan, and Mumbai.
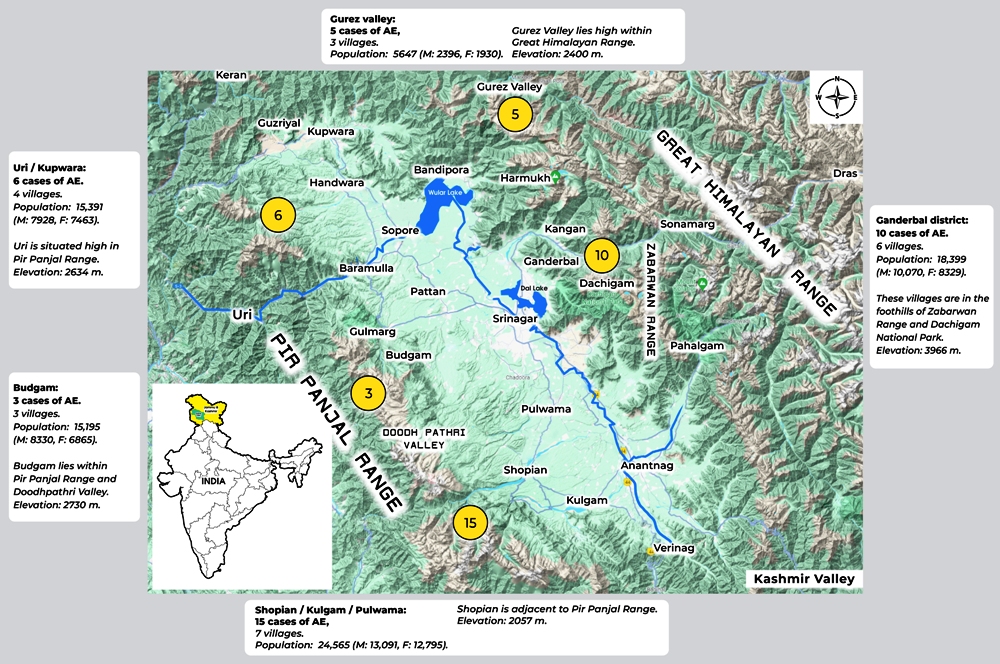
Impressed by the magnitude of AE in Kashmir, we envisaged further defining the prevalence, incidence, and burden of Disease AE namely DALYs in Kashmir. Crucial for all this was determining the population in which the infection existed in Kashmir. We had contact details of 39 AE patients from Kashmir, including 12 cases from DKMC and 27 cases retrieved from other Kashmir and North India centres. On scrutiny, these patients resided in 22 villages with a total population of 79,197 from five peripheral districts of the Valley (Fig 5). Of significance, none of the patients at the time of scrutiny belonged to the Kashmir valley bottom, and there was no case from other parts, namely Kargil, Ladakh, or Jammu. Based on these data, we believe there were around 10 incident cases of AE per year in Kashmir with a prevalence of 146.47/105 and an incidence of 12.41/105/year. We used a model with standard assumptions to calculate the Burden of Disease of AE in Kashmir. The assumptions included applying a disability score of 0.3 for AE as is applied for HCC; AE is uniformly fatal in eight years if left untreated, and the Indian population’s life expectancy is 2050. The total number of DALYs for AE in Kashmir, India, is 3100.56. Here, I must mention that one DALY means the loss of one year of a healthy life.
How do these data compare with published data on AE globally? The disease is highly endemic in China, amounting to over 95 per cent of the world infection load. Other regions with high endemicity include Turkey and central Asian republics, such as Kazakhstan, Kyrgyzstan, etc. I believe the endemicity of AE in Kashmir is akin to these regions in Central Asia as of today.

Suggestions
I propose critically evaluating this evolving, emerging, and exploding important health problem in Kashmir. Due to its geographical and ecological features, Kashmir is and will remain an ideal location for the existence of AE. Altitudes, parks, sanctuaries, forests, and climate are suitable for maintaining the Sylvatic cycle in wild animals, namely the Kashmir red fox.
Human exposure occurs in people who live or visit high altitudes, work or visit parks and wildlife sanctuaries, eat wild fruit, chew grass, or are involved in haymaking. Dogs, as a definitive host in an urban cycle of E. multilocularis, can potentially cause community spread of infection in the future. The emergence of AE in Kashmir needs a plausible explanation. Over the decades since 1980, several phenomena have culminated in the emergence of AE in Kashmir. The most significant are massive deforestation and urbanization and the contraction of the habitat of the definitive host. Kashmir red fox is highly accommodative to human dwellings, and the fox has shifted from altitudes to gardens and localities in peripheral regions for food.
While so, we built orchards in the foothills of the Himalayas in Shopian and Ganderbal to invite the host. Another important factor may be social unrest leading to a more frequent movement to forests and climate change causing latitude and altitude shifts of small mammals, namely rodents. Several important steps need to be taken to address this evolving human threat to Kashmir and adjacent regions. These include continued surveillance, determining the potential risk factors for spreading and addressing their control. Of course, molecular studies are necessary to trace the origin of infection and develop clinical units to manage this complex disease.
Finally, a matter of concern! E. multilocularis infection in Kashmir is currently passing through a sylvatic cycle. The definitive host is a wild animal, the Kashmir Red Fox and human exposure is limited to peripheral mountainous regions. The real danger is the change to an urban cycle where the dog becomes the definitive host. If this happens, there will be a community spread, and we will start seeing cases from the Kashmir basin and other regions as well.
(Dr Khuroo, MD, DM, FRCP (Edin), FACP, and Master of the American College of Physicians (Emeritus), has held numerous prestigious positions including Dean and Director of SKIMS and Ex-officio Secretary to the Government, Professor and Head of Gastroenterology and Chairman of the Department of Medicine at SKIMS, Consultant and Head of Gastroenterology and Liver Transplantation at KFSH&RC in Riyadh, and currently serves as the Director of the Digestive Diseases Centre at Dr Khuroo’s Medical Clinic (DKMC) in Srinagar.)













