
Acclaimed scientist, Prof Mohammad Sultan Khuroo’s significant contribution include the discovery of Hepatitis-E virus in 1978 from Kashmir when 1700 of an estimated 52000 cases of icteric hepatitis, cases died. In an interview to Syed Samreen, Khuroo terms Coronavirus a python, asserting only powerful drugs and a vaccine can break the transmission chain
KASHMIR LIFE (KL): Coronavirus pandemic has stopped the world in its tracks. What makes the virus more contagious than its previous strains?
PROF MOHAMMAD SULTAN KHUROO (MSK): The Coronavirus infection which originated from Wuhan, China in December 2019 has turned into a global catastrophe. The virus causing the disease has been designated as Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2) and the disease caused by the agent as Coronavirus Disease-2019 (COVID-19). WHO pronounced the disease as a pandemic on March 11, 2020. SARS-CoV-2 belongs to a family of zoonotic viruses known as Coronavirus with the genus Betacoronavirus and is closely related to two other viruses namely Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and the Middle East Respiratory Syndrome Coronavirus (MERS-CoV).
All three are bat viruses and cross over to cause human infection through an intermediate host (civets for SARS-CoV, camels for MERS-CoV, and possibly pangolins for SARS-CoV-2). SARS-CoV epidemic occurred between November 2002 to July 2003 and originated from Beijing and spread to 29 countries resulting in infection to 8096 people with 774 deaths, fatality rate of 9.6%. MERS-CoV epidemic occurred in late April to May 2013 in Al-Hasa, Saudi Arabia, spread to Arabian Peninsula and South Korea and resulted in 2494 infections with 858 deaths, a case fatality rate of 34.4 % (15-17). In contrast, SARS-CoV-2 has a case fatality rate of 2.3%, with higher rates among elderly patients and patients with co-morbidities.
Coronaviruses resemble each other and are enveloped viruses, around 125 nm in diameter, with a positive-sense single-stranded RNA genome of around 30kb.
While the three viruses are from the same family, they have two distinct differences. SARS-CoV-2 has the sequence (nucleotide) the resemblance of around 80% to SARS-CoV and around 50% to MERS-CoV. Also, the spike protein of SARS-CoV-2 has the receptor-binding domain (RBD-the site which attaches to the ACE2 receptors) highly optimized for binding. It can bind to ACE2 receptors many times more powerfully than for the other two Coronaviruses. This is the main reason for the extremely high infectivity of the SARS-CoV-2 and the extraordinary spread of the disease in the community.
KL: What do you think is the origin of the Coronavirus? Is it man-made or natural?
MSK: Thank you for asking this important question. The question has political overtones as many Governments (the USA in particular) and even many researchers have asserted that the virus originated in a Chinese lab due to deliberate manipulation and accidental leak rather than from the seafood wholesale market, as reported by Chinese agencies. Theoretically, it is possible that viruses while passing repeatedly through cell cultures, for example, laboratory manipulation, can mutate and evolve. However, for that, we need to have a progenitor which is not known as of today or has not been found. It is a remote possibility that the evolved virus will adapt to human host with such extraordinary properties as in SARS-CoV-2.
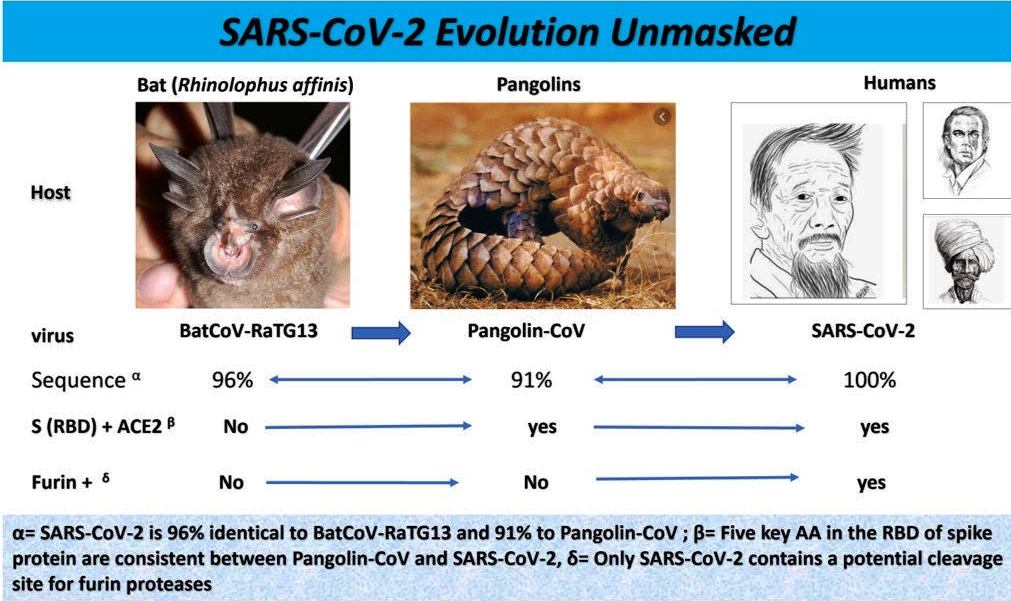
Next, SARS-CoV-2 cannot originate and evolve from SARS-CoV and Mers-CoV as both have low sequence resemblance (50 to 80%) with the virus. The investigators have identified another Coronavirus named as BatCoVRaTGI3 from bats (Rhinolophus affinis), which has close sequence similarity with SARS-CoV-2. It is likely that this virus is the progenitor of SARS-CoV-2. However, this virus lacks the RBD in the spike protein which is pathognomonic of SARS-CoV-2. To fill this gap pangolins are known to be infected with a Coronavirus which closely resembles BatCoVRaTG13 and SARS-CoV-2 and also has RBD (though less potent) in the spike protein. So, it was postulated that SARS-CoV-2 could evolve and jump to humans through an intermediate host, namely the pangolins.
The virologists have used a special technology called Phylogenetics to study the origin, evolution, and global spread of viruses. Recently, a phylogenetic network analysis of 160 complete human genomes of SARS-Co-2 (reported from all over the globe) was done. Based on the study, it was concluded that SARS-CoV-2 originated from BatCoVRaTG13 and evolved into 3 strains (A, B, and C) and spread globally. Thus, as of today, there is impending evidence that SARS-CoV-2 has evolved through natural variation so common in RNA virus replication in bats and jumped to humans through an intermediate host, namely pangolins. The evidence for deliberate laboratory manipulation and an accidental leak is on weak ground.
KL: Why is the virus is called a ‘Corona’ virus? How does washing hands with soap help?
MSK: Corona’s name comes from the appearance of the virus under an electron microscope. SARS-CoV-2 is a spherical coated virus and has several proteins on the surface. These include n-protein, E-protein, and S-protein. The S (spike protein) is attached to the nucleocapsid in the form of multiple clubs projecting outwards. The spike protein attaches to ACE2 receptors cause fusion and entry in the cell. The spike protein clubs on an electron microscope gives the shape of the solar corona to the virus.
Soap is a detergent and dissolves all fats and greases. The virus has a fat covering and washing hands for 20 seconds dissolves the fatty layer of the virus, disintegrates the particle and inactivates the virus. So, kindly be informed that washing hands with soap for 20 seconds is a highly effective method to block virus transmission and must be practised frequently.
KL: What are the symptoms of the disease? When should we worry?
MSK: COVID-19 has an incubation period or 2 to 14 days and presents with fever with shaking chills, dry cough, and fatigue with aches and pains. Anosmia (loss of smell as well as taste) may occur. Most patients recover over a matter of days to a week. An undefined percentage of subjects infected with the virus may have no symptoms. Such subjects have the virus in the throat and nose and can spread the disease to others if protective measures are not taken. A small percentage of patients present with alarm symptoms which include continued high fever and shortness of breath. Such patients need urgent medical attention and hospital admission. Pneumonic illness due to COVID-19 is caused by an inflammatory response in the lungs and the production of cytokines. Such patients cannot maintain the oxygen concentration in the blood and need assistance by high flow nasal oxygen and in small subset intubation and ventilation.

Although lungs are the primary targets of COVID-19, sick patients can present with varied bizarre manifestations. These include involvement of heart with heart attacks in young people, the involvement of blood vessels causing low blood pressure and large blood clots in the vessels, kidney involvement causing renal failure needing dialysis. Skin disease can resemble chilblains (COVID toes) and the involvement of the brain can cause delusions and strokes. Abdominal pain, loss of appetite, vomiting, and diarrhoea are common with chest symptoms. The virus is excreted in faeces and may infect others through the faecal-oral route. Children present with multisystem inflammatory syndrome causing skin rashes like scarlet fever with inflammation of arteries and heart resembling Kawasaki disease or toxic shock syndrome.
KL: There is a steep rise in the number of cases in Kashmir despite the lockdown. What do you think is going wrong?
MSK: COVID-19 is a disease with the extra-ordinary potential of human-to-human transmission through droplets generated with coughing and sneezing. It gets deposited on surfaces and can survive there for hours and be transmitted through hands and fomites when we touch mouth, nose, or eyes. Evidence is accumulating that SARS-CoV-2 maybe spread through aerosol (micro-particle in the air) and if proved, it shall resemble measles virus which has the number one potential to spread in the community. Faecal-oral transmission of SARS-CoV-2 is a possibility as a virus is excreted in faeces. The disease has caused massive death and devastation.
To fight this python, we need powerful weapons that include powerful and highly effective drugs to treat and prevent infections or a highly effective, safe, and affordable vaccine to break the transmission chain. As of today, we lack either. The diseases like AIDS and HIV infections, major killers of humanity, are being fought with highly effective antiviral drugs. Smallpox, a major killer disease has been eradicated with the availability of a highly effective vaccine.
To compensate for the absence of a drug or a vaccine, we are fighting this pandemic with lockdowns, social distancing, hand washing, surgical masks and quarantine to prevent the human-to-human spread of the virus. This has adversely affected productivity, public freedom, and social order and resulted in global economic devastation. However, we have to be realistic that these are mitigation measures and shall reduce the morbidity and mortality caused by the virus, but can never compete with what a drug or vaccine can do. It is impossible to completely block human transmission through mitigation procedures. Though we have gained tremendously by these methods and reduced the impact of the disease in the community, the virus transmission cannot be blocked cent per cent. A large proportion of the population who were caught up outside Kashmir in the time of lockdown have to be allowed to come back to their homes. Such practice shall cause small temporary outbursts of new infections. However, the quarantine policies of the Government effectively cover this risk.
KL: Do you endorse Hydroxychloroquine for prophylaxis and treatment of COVID-19?
MSK: Of all the potential therapies, Chloroquine and Hydroxychloroquine have been the focus of tremendous public attention. There have been sharp differences in opinion as to the role of these two drugs in the prevention and treatment of SARS-CoV-2 infection. On one extreme, these drugs have been touted as “biggest game-changers in the history of medicine”, while at the other end these drugs have been trolled as “useless and dangerous” Both drugs have been used in the treatment and prophylaxis of malaria and long-term use of Hydroxychloroquine is the cornerstone in the treatment of several auto-immune disorders.
There is convincing evidence that Hydroxychloroquine has strong in vitro antiviral activity against SARS-CoV-2. Few small uncontrolled trials and several anecdotal reports have shown conflicting results of such drug therapy in COVID-19. However, as of today, the results of large scale randomized controlled trials have not shown a beneficial effect on COVID-19. Despite this, Hydroxychloroquine is used as a desperate attempt for prophylaxis and treatment of COVID-19. The drug has wide-ranging drug interactions and potential cardiotoxicity, especially when co-administered with Azithromycin. The drug is known to prolong the QTc interval. This is due to the drug-related block of the inward rectifier potassium ion channel (Kir2.1). Drug-induced QT/QTc per se is asymptomatic. However, it can lead to Torsades de Pointes (TdP), a potentially lethal polymorphic ventricular tachycardia. Patients with TdP present with episodes of near syncope, syncope with or without convulsions, and sudden cardiac death. Indiscriminate unsupervised use can expose the public to serious adverse drug effects. Based on the evidence available as of today, I do not endorse the use of Hydroxychloroquine for prophylaxis or treatment of COVID-19.
KL: What is the status of the vaccines against COVID-19?
MSK: There has been an unprecedented fast track path taken in Research and Development (R&D) by the world community for developing candidate COVID-19 vaccines. As on May 5, 2020, the global COVID-19 vaccine R&D includes 108 candidate vaccines. Until now, several candidate vaccines have completed the exploratory and preclinical stage, obtained Clinical Trial Authorization, and initiated recruitment of volunteers for clinical trials. Of these six candidate vaccines stand at the forefront of clinical trials. These are Ad5-nCoV from CanSino Biologicals Inc, mRNA-1273 from Moderna, PiCoVacc from Sinovac Biotech, ChAdOx1 from the University of Oxford, BNT162 (a1, b1, b2, c2) from BioNTech and INO-4800 from Inovio.
Even with a tremendous race against time to develop a vaccine, one has to appreciate that clinical trial to define the efficacy and safety of the vaccine is the greatest time-limiting factor. Given the urgency, many essential steps in clinical trials are being bypassed by simultaneous phase I-II trials and obtaining efficacy data from phase IIb trials. I believe challenge studies may be allowed and if so, we shall have one or more vaccines available by the fall of 2020. With all this, vaccine developers are ready to scale up manufacturing capacity to massive demands once the product is allowed for marketing. However, concerns are raised about a rush to deploy a COVID-19 vaccine. Applying Quick Fix and short cuts can lead to errors with disastrous consequences. We need to keep our fingers crossed and hope for the best.













